
Pelvic Inflammatory Disease!



Pelvic Inflammatory Disease(PID) Diagnosis And Treatment
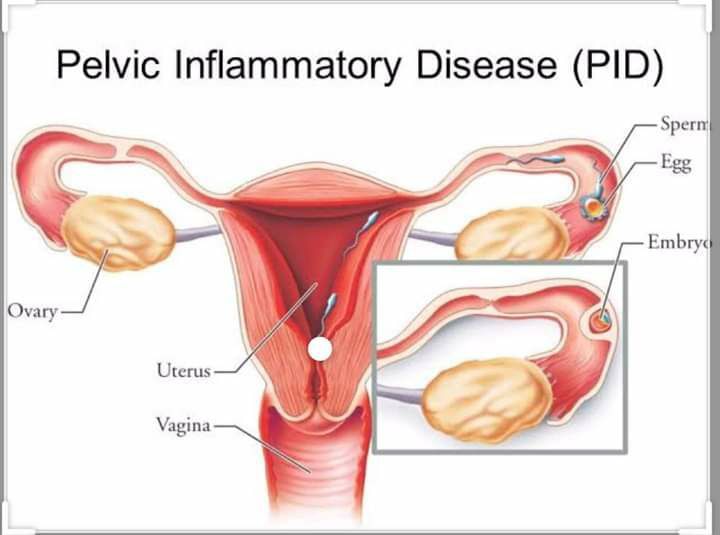
Definition
PID is defined as an infectious disease of the upper female reproductive system. This infection usually affects the uterus, fallopian tubes and, in some patients, the ovaries. Pid is closely linked with sexually transmitted diseases and the most commonly implicated organisms are chlamydia trachomatis, neisseria gonorrhoeae, and gardnerella vaginalis. Approximately, 20% of women who are untreated for chlamydial and gonorrheal infections will develop PID. Viral infections can also complicate pid and they includeherpes simplex type 2 and cytomegalovirus.
Several risk factors
- Multiple sexual partners
- Previous history of sexually transmitted infections
- Invasive gynecological procedure such as an endometrial biopsy.
- Intrauterine devices for contraception
- Clinical presentation of pelvic inflammatory disease
Patients, if symptomatic, usually present with a fever, nausea, vomiting and pelvic and abdominal pain. Several clues exist that can make the physician suspect pelvic inflammatory disease as the etiology of abdominal pain in a young female patient, which include multiple sexual partners, a recent history of a sexually transmitted infection or the use of an intrauterine device for contraception.
Patients usually present during their menstruation, another clue towards pid as the cause of abdominal pain.
Pelvic pain is exacerbated by intercourse, motion or exercise. PID, if untreated, can lead to intraabdominal abscess formation or infertility, hence the threshold to diagnose pid should be low. Accordingly, any patient who presents with the above picture should undergo an abdominal and pelvic examination looking for any of the following three signs:
(1) cervical motion tenderness
(2) uterine tenderness
(3) adnexal tenderness
Diagnosis
- Laparoscopic confirmation
- Oral temperature above 38.3 c
- Abnormal cervical or vaginal discharge
- White blood cells on microscopic examination of the vaginal discharge
- Elevated erythrocyte sedimentation rate and
- (CRP) c-reactive protein level
Laboratory confirmation of chlamydia or neisseria gonorrhea infection by dna.
The presence of
- Fever
- Lower abdominal pain
- Vaginal discharge
- And a high erythrocyte sedimentation rate is usually enough, and the other criteria are only there to increase the certainty.
Laboratory investigations are needed to exclude other differential diagnoses and to confirm the diagnosis. The presence of more than 10 white blood cells per high-power field on microscopic examination of the vaginal secretions is a good diagnostic criterion for pid. Additionally, the detection of chlamydia or gonorrhea dna or culture studies can be helpful in increasing certainty.
Leukocytosis is found in about 50%
Transvaginal ultrasonography such as an
Abscess orectopic pregnancy.
Treatment of (PID)
- Ceftriaxone
- Doxycycline
- Metronidazole
Or
- Cefoxitin
- Doxycycline
- Metronidazole
Treatment
Ceftriaxone 250 mg I'm + Doxycycline 100 mg po bid x 14 days
If concern for anaerobic cause consider adding
Metronidazole
Another possible and acceptable regimen for treatment includes
Clindamycin iv and Gentamicin iv
Like the previous treatment, 24 hours after clinical improvement, the patient should start taking doxycycline orally for two weeks.



+1.svg)
